


While researchers once thought osteoarthritis to be a disease restricted to the articular cartilage lining the ends of long bones inside joints, they now consider it a whole-joint disease. Specifically, inflammation within any of the joint tissues secondary to trauma (i.e., repeated concussion during exercise) can set off a cascade of molecular events that lead to:
- cartilage degradation
- inflammation, hyperplasia (abnormal increase in cell number), and hypertrophy (in size) of the inner lining of the joint, called the synovium
- joint capsule thickening or fibrosis
- bone changes, such as a hardening of the bone layer lying directly beneath the articular cartilage (i.e., subchondral sclerosis). In addition, bony growths called osteophytes can also form on the edges of bones near the joints.
Clinically, horses with arthritis could experience heat, pain, and swelling localized to one or more joints. However, some horses might not show overt clinical signs.

Osteoarthritis is the leading cause of lameness in horses, responsible for approximately 60% of all lameness cases (as cited by Aragona et al., 2024). The condition drives attrition and early retirement in horses and ultimately leads to welfare issues in severely affected individuals.
Some of the pain from OA is nociceptive, caused by loading the joint that stimulates the sensory pain fibers. As OA further progresses, it often leads to chronic pain that can trigger neuropathic conditions—where nerve damage worsens pain—or maladaptive changes, which are lasting nervous system changes that continue to cause discomfort even after the initial damage has subsided. More specifically, damage to neurons innervating the joint, causing pain independent of the joint pathology’s (disease or damage) severity, might occur (McKenzie et al., 2023; Eitner et al., 2017).
Before delving into how to treat OA-related pain, the first step is recognizing musculoskeletal discomfort in horses.

The traditional pain scale veterinarians use in the United States for evaluating lameness in horses is the American Association of Equine Practitioners’ (AAEP) Lameness Scale, which allows them to subjectively grade horses on a scale from 0 (no lameness) to 5 (minimal weight-bearing).
This scale has its limitations. Notably, not all horses with OA show up with a hobbling gait. Instead, signs of pain can be quite subtle and, therefore, missed using this tool.
Therefore, equine veterinarians developed other approaches to more reliably identify musculoskeletal pain—even subtle pain due to mild OA. These include body-mounted inertial sensor systems (BMIS) and force-plate analysis. While useful, these latter techniques require specialized equipment that is not readily available or often too costly for daily use in equine practice. Further, the results with bilateral lameness—mentioned earlier, when the horse is lame in both limbs of a pair—might be misleading.
This is where pain scales could be useful. Practitioners have several available for clinical use, including the horse grimace scale seen below, the Equine Utrecht University scale of facial assessment of pain (EQUUS-FAP), the equine pain scale (EPS), the Equine Brief Pain Inventory (EBPI), the composite orthopedic pain scale, and the horse chronic pain scale.

However, Dyson says these pain scales were designed for use in horses at rest, not during exercise.
“Further, these scales have shown limited efficacy in the identification of chronic musculoskeletal pain so far,” she adds.
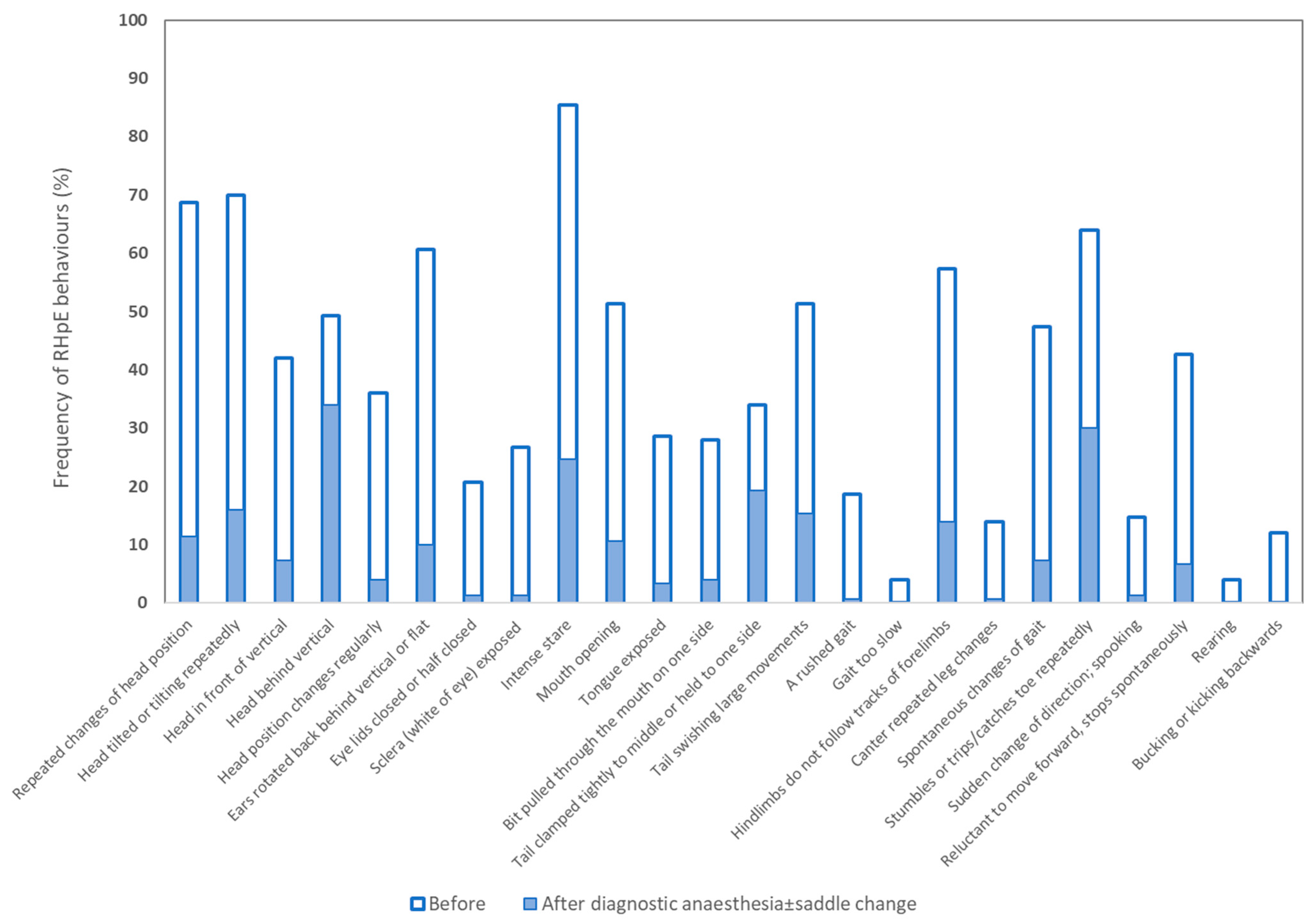
Hoping to fill the need for a tool capable of recognizing musculoskeletal pain in ridden horses, Dyson and colleagues unveiled the ridden horse pain ethogram (RHpE) in 2017. The RHpE is a collection of 24 behaviors, the majority of which are at least 10 times more likely to be seen in a lame horse than a nonlame horse (Dyson, 2022; Dyson and Pollard, 2023; Dyson and Pollard, 2024).
Examples of these behaviors include:



Despite a large proportion of horses not appearing conventionally lame, the median RHpE score was 9 out of 24 (with the range being 2-15), which decreased to a median of 2 out of 24 (range 0-12) following blocking.

Back in 2014 researchers published an article about the current knowledge surrounding pain control in horses. “Currently, approaches to pain control in horses lack a robust evidence base,” the authors, Sanchez and Robinson, wrote. “Although research reports of antinociceptive and analgesic (pain-killing) therapy in horses have certainly gained ground over the years, most involve models of healthy horses or retrospective evaluation of clinical cases. Reports of prospective clinical trials are few and far between; thus, most practitioners base analgesic choices upon a combination of the available literature and clinical experience.”

Today the situation remains similar. But here we’ll briefly describe many of the oral pharmaceuticals available for managing chronic pain in horses, addressing the benefits of each while noting some potential drawbacks/adverse effects.


This medication, classified as a nontraditional NSAID, primarily exerts analgesic effects through pathways not involving COX enzymes.
“I am definitely seeing acetaminophen being used more frequently in our region, but that may be because we have worked on communicating its utility to our referring veterinarians,” says McKenzie. “This drug is certainly not the answer to all of our problems, but I do think it has efficacy and true clinical utility, especially when used in combination with other drugs.”

Perhaps the drug with the greatest enthusiasm behind it of late is CBD (cannabidiol) derived from the hemp plant Cannabis sativa. This interacts with the endocannabinoid system that regulates nociception and inflammation.
In 2024 Interlandi et al. evaluated the efficacy of CBD in 20 horses with mild fetlock OA. They found that horses supplemented with CBD had significantly lower heart rates and respiratory rates, as well as Horse Chronic Pain Scale scores.
“The addition of a cannabidiol-based product to an analgesic protocol was well tolerated and showed positive effects on the treated subjects, improving their quality of life and pain relief,” said the researchers.
Dr. Laurie Goodrich, professor of surgery and lameness at CSU’s Johnson Family Equine Hospital, says horses with OA need to keep moving. When horses stop exercising in the face of OA, their joint capsules become fibrotic, and that fibrosis causes more pain, which limits the horse’s ability to exercise.
“It’s a negative feedback loop,” says Goodrich. “We cannot just let the horse sit and rest.”
The type of exercise a horse with OA needs depends on the specific joint and the severity of disease.
“Rehabilitation may include flexion and extension exercises, but truly there is no blanket protocol for these horses,” says Goodrich. “Owners need to work with their veterinarian and a certified rehabilitation specialist.”

She says she believes an underwater treadmill is great for arthritic horses.
“With the water there are a lot less direct mechanical forces on the joints, and ligaments and tendons can get exercised without those forces,” Goodrich explains. “Many rehabilitation programs with treadmills aren’t cheap but worth it, allowing horses to continue exercising.”
When choosing a rehabilitation specialist, Goodrich advises looking for centers operated by a diplomate of the American Association of Veterinary Sports Medicine and Rehabilitation. These types of facilities operate around the country and should be considered before using uncertified individuals.
And not to be overlooked is the effect of obesity on joint health. According to Pratt-Phillips and Munjizun (2023), “Excess body weight has been documented to affect gait quality, cause heat stress and is expected to hasten the incidence of arthritis development.”

Stacey Oke
 Stacey Oke, MS, DVM, is a practicing veterinarian and freelance medical writer and editor. She is interested in both large and small animals, as well as complementary and alternative medicine. Since 2005 she’s worked as a research consultant for nutritional supplement companies, assisted physicians and veterinarians in publishing research articles and textbooks, and written for a number of educational magazines and websites.
Stacey Oke, MS, DVM, is a practicing veterinarian and freelance medical writer and editor. She is interested in both large and small animals, as well as complementary and alternative medicine. Since 2005 she’s worked as a research consultant for nutritional supplement companies, assisted physicians and veterinarians in publishing research articles and textbooks, and written for a number of educational magazines and websites.



